


What happens when we the parents die? Insights from the 2025 UJA of NYC Hilibrand Autism Symposium
Keynote Speaker Marsha R. Mailick, Ph.D. and Professor at the University of Wisconsin-Madison

Images with permission and courtesy of @EKO LOVES YOU on X, and on Substack.
I recently attended the UJA’s 18th Annual Hilibrand Autism Symposium. Beth Rosenberg is the Project Consultant for the event, and she is a parent of a neurodiverse young man. Beth also runs Tech Kids Unlimited, and the entire agenda for the day can be found here. I want to focus on the Dr. Marsha Mailick presentation. It was an eye opener.
I am guilty of it. I still think of Dustin Sweeney as my child:
Dustin is NOT a child now. He is a 27 year old man and it time for ME to really discuss the BIG question:
What happens when we, the Parents, die?

“Healthy aging and a long life are hopes and goals that everyone shares. Extending these hopes and goals to autistic adults is vitally important. We collectively have a responsibility to ask difficult questions, carefully study the data, and reach a new understanding of autism during midlife and old age. These are stages of life that have largely been unexplored for people diagnosed with autism and it is time to make this our priority.”
Marsha R. Mailick, PhD

Marsha R. Mailick, PhD is the Emeritus Vice Chancellor for Research and Graduate Education at the Waisman Center at the University of Wisconsin which is “advancing knowledge of human development, developmental disabilities, and neurodegenerative diseases”. Marsha’s bio and research portfolio are here.
Marsha’s Hilibrand presentation was listed as “Aging With Autism: Functional, Health, and Employment Outcomes in Mid- and Later-Life” and “will examine the unique challenges and opportunities encountered by autistic individuals as they navigate aging. It will highlight critical aspects of adulthood to offer insights into forging a sustainable and fulfilling path forward.”
Marsha stated to me in a followup exchange: “The data we analyzed in our study included some autistic people who died BEFORE the death of their parents as well as others who died AFTER.
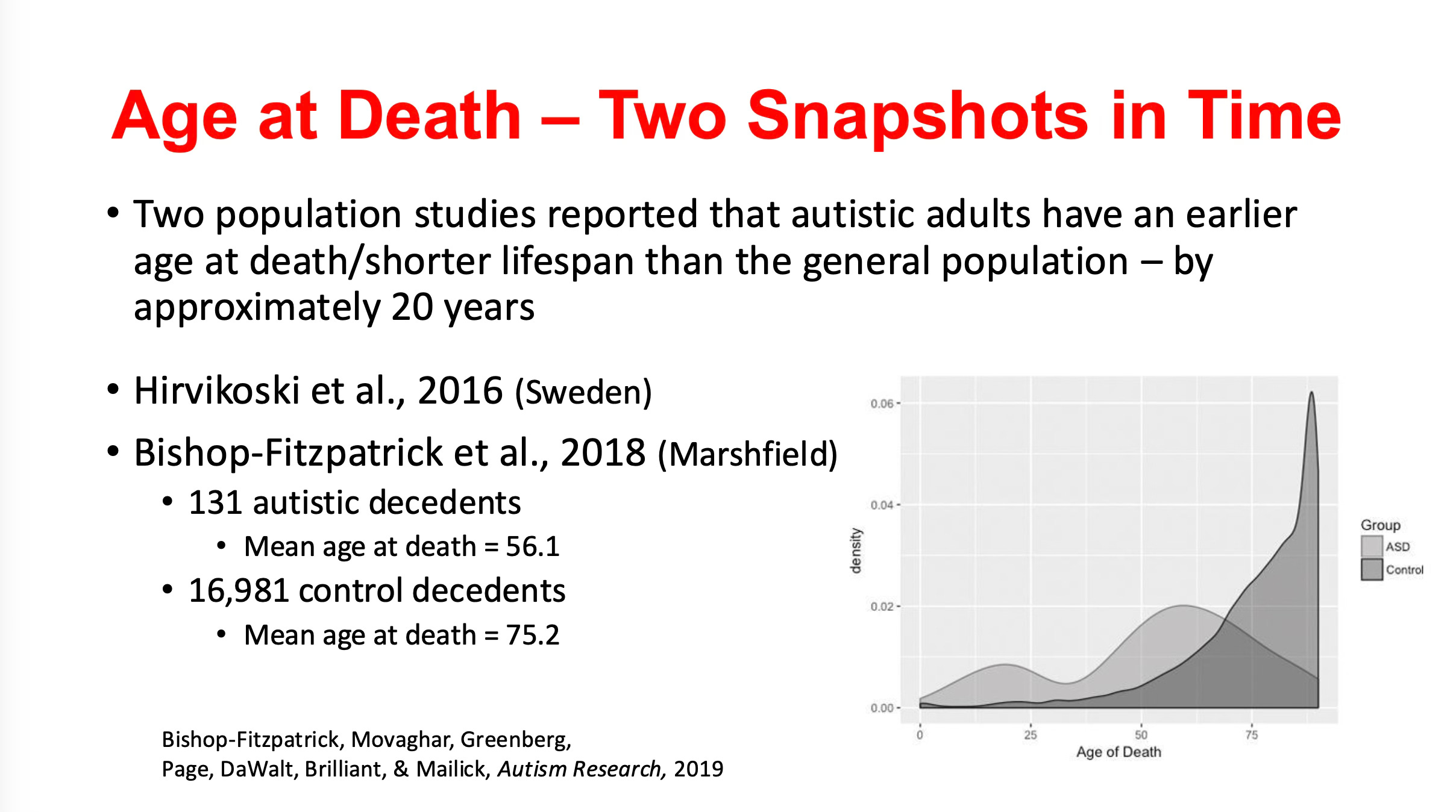
So the obvious question is, “Why are Autism Adults dying 20 years earlier?
My simplistic answer after listening to Marsha’s presentation is the adults in her study and the Swedish study may have gotten kicked back into a system that was not built for middle age, and certainly not old age. There appeared to be a correlation to the Parents dying, but there were many factors.
Marsha also offers solutions:
It’s time for Parents to connect. Nobody is going to fix this for us. 20 years is an enormous gap.

Many of the CommHab Workers, Staff, and Community that surrounds Endeavor 21+ Foundation (Dustin Sweeney’s community in Chestnut Ridge, NY) have lived “In Community”, which is a Threefold/Steiner/Camphill philosophy. Steiner’s belief was that communities should address practical needs (education, health, agriculture) while nurturing spiritual and social connections.
Ken Siri, Support Broker to Dustin Sweeney, and Father to Alex Siri stated:
Besides working to improve our own health/longevity as a parent, we need to cultivate a real Circle of Support (COS). I have ideas on this including having a team of brokers (strategic, tactical, emotional), creating regular social interactions between a person and their own stakeholder community, and parties/events focused on the person and including their whole stakeholder community.
Cayle White of the JCC Manhattan and a Sibling Advocate added:
And it should not just include the agencies and family members We should expand to volunteers, friends, and neighbors should be part of the planning.


Why Autistic Adults Are Dying Approximately 20 Years Earlier on Average:
(I used @Grok for this section, with edits by Mike. Artificial Intelligence was an amazing tool for this piece. Marsha helped me with the edits, but it was a really good summary draft.)
Based on the Marsha R. Mailick presentation from the UJA Hilibrand Conference and her research, several factors contribute to the reduced lifespan of autistic adults, with an average age at death around 56.1 years compared to 75.2 years for non-autistic controls (a roughly 20-year gap). Key reasons include:
Higher Burden of Disease:
Autistic adults have a significantly higher prevalence of health conditions across seven domains: cardiovascular, endocrine, gastrointestinal, neurological, nutritional, psychiatric (other than autism), and sleep disorders. This increased disease burden, particularly pronounced in autistic women, likely contributes to earlier mortality.
The document highlights that autistic adults have more diagnostic codes entered into electronic health records (EHRs) across these domains compared to matched non-autistic controls.
Predictors of Mortality:
Limitations in Activities of Daily Living (ADL): Lower ADL skills (e.g., self-sufficiency in hygiene, meal preparation, financial management) at the start of the study were associated with an 8% increased risk of death per 1-point decrease on the ADL measure.
Impairments in Social Reciprocity: Greater impairments in social reciprocity during early childhood were linked to a 23% increased risk of death per 1-point increase in impairment. These factors, measured earlier in life, suggest long-term impacts on health outcomes.
Age and overall health status also predict mortality, but ADL and social reciprocity remain significant even when controlling for these.
Causes of Death:
In the Adolescents and Adults with Autism (AAA) study, causes of death included cardiac issues (6 cases), cancer (5), respiratory issues (5), seizures (5), accidents (4), medication side effects (2), and unreported causes (11). These reflect a mix of chronic health conditions and acute events, some potentially exacerbated by autism-related challenges.
Potential Barriers to Healthcare:
The document raises the question of whether these patterns result from autism itself or barriers to accessing healthcare, such as difficulties in communication, sensory sensitivities, or inadequate provider training. These barriers may lead to delayed diagnoses, untreated conditions, or inappropriate care.
Polypharmacy is commonly defined as the use of five or more prescription medications. Data from the National Health and Nutrition Examination Survey (NHANES) between 1988 and 2010 found that the proportion of ALL adults aged 65 and older taking five or more prescription medications tripled from 12.8% in 1988–1991 to 39.0% in 2009–2010. More recent data from NHANES, covering 1999–2018 indicate this figure had risen to 44.1% for those aged 65 and older.
Autistic adults experience an accelerating increase in prescription medications (both psychotropic and non-psychotropic) after midlife, raising risks of drug interactions and side effects, which may contribute to mortality (e.g., two deaths in the AAA study were linked to medication side effects).
Social and Environmental Factors:
Social isolation, reduced social engagement, and loss of support systems (e.g., family members aging or passing away) may exacerbate mental and physical health issues. For example, the case study of Teresa illustrates how losing a job, a lifelong friend, and a parent correlated with increased behavioral problems and social isolation.
Accelerated Aging:
The document notes that midlife (30s and 40s) is a turning point where autistic adults experience declines in behavioral health, ADL self-sufficiency, social engagement, and increased polypharmacy. This suggests an accelerated aging process, potentially due to chronic stress, stigma, or biological factors associated with autism.
What Can Be Done to Address This?
Marsha’s research proposes several strategies to enhance healthy aging and potentially extend lifespan for autistic adults, with a focus on midlife as a critical period for intervention:
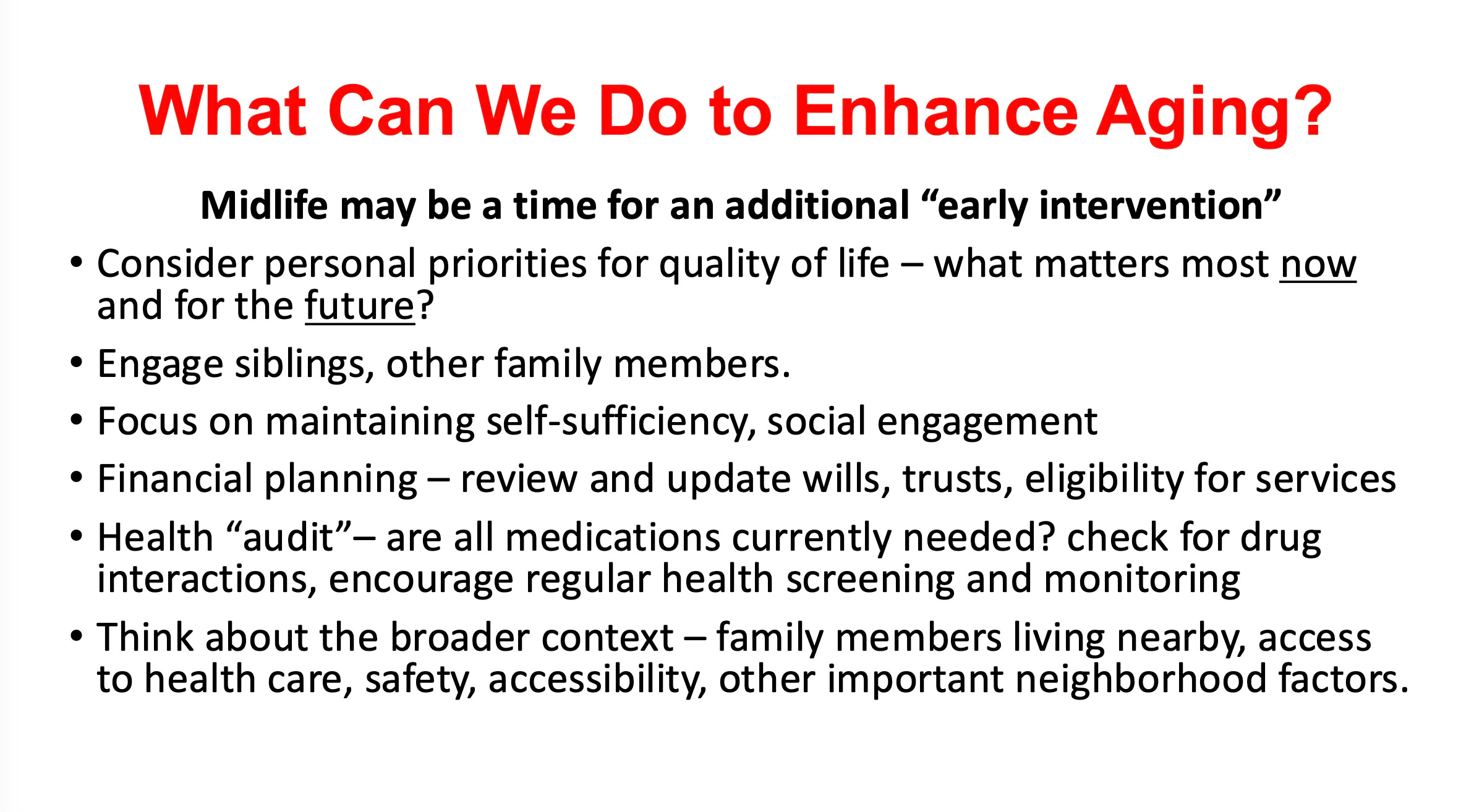
Midlife "Early Intervention":
Implement targeted interventions in midlife to address declining health, self-sufficiency, and social engagement. This could include programs to maintain ADL skills, promote physical activity, and manage chronic conditions.
Encourage regular health screenings and monitoring to catch and treat conditions early.
Health Audits and Medication Management:
Conduct a thorough review of all medications to assess necessity, check for drug interactions, and minimize side effects. Reducing polypharmacy risks is critical given the increased use of medications in midlife.
Promote regular health check-ups tailored to the needs of autistic adults, considering sensory sensitivities and communication challenges.
Enhancing Self-Sufficiency and Social Engagement:
Develop programs to maintain or improve ADL skills, such as training in personal hygiene, meal preparation, or financial management.
Foster social connections through community programs, peer support groups, or activities tailored to autistic adults’ interests and sensory needs. This could mitigate the impact of social isolation, as seen in Teresa’s case.
Improving Healthcare Access:
Train healthcare providers to better understand autism, including how to accommodate sensory sensitivities, communication differences, and atypical presentations of symptoms.
Advocate for systemic changes to reduce barriers, such as providing longer appointment times, using visual aids, or involving caregivers in medical discussions.
Family and Community Support:
Engage siblings and other family members in planning for the future, especially as parents age or pass away. This includes financial planning (e.g., updating wills, trusts, and service eligibility) and ensuring a support network.
Assess the broader context, such as proximity to family, access to healthcare, neighborhood safety, and accessibility, to create a supportive environment.
Targeting Modifiable Risk Factors:
Focus on improving ADL skills and social reciprocity early in life, as these are predictors of mortality. Early interventions could include social skills training, occupational therapy, or life skills programs.
Address chronic stress and stigma through mental health support, counseling, or community inclusion initiatives.
Research and Policy Advocacy:
Prioritize research on why autistic adults experience accelerated aging and higher disease burden. This includes studying biological, environmental, and social factors.
Advocate for policies that improve access to services, employment opportunities, and healthcare for autistic adults, especially as they age.
Investigate how patterns of aging may differ for newer generations of autistic individuals who benefit from early interventions and better services.
Support for Loss and Grief:
Develop resources to help autistic adults cope with significant losses (e.g., death of a parent, loss of a job, or social connections). This could include counseling, support groups, or structured activities to process grief.
By addressing these factors through targeted interventions, improved healthcare access, and robust support systems, it may be possible to reduce the lifespan gap and enhance the quality of life for autistic adults as they age.
Dustin has purpose in his life via his work - Threefold Cafe, Threefold Community Farm, Central Park Green Team, and Artis Senior Community. Now we are looking at ways to make it sustainable by improving his Spelling/Communication skills at The Invictus Observatory.
#AeternusUmbra (watch forever)

This is really needed. What these kids and parents face as they both age